All published articles of this journal are available on ScienceDirect.

Cervical Abscess in the Newborn: About Two Cases
Authors Info & Affiliations
Abstract
A cervical abscess is defined as a collection of pus in the structures of the neck, sometimes called deep neck infection or neck abscess. It is unusual in neonatal period. In this paper, the authors present two cases of neonatal neck abscess admitted in the neonatal intensive care unit of Mohammed VI University Hospital, Marrakesh (Morocco). The first case is caused by a neonatal infection; the second case is post-traumatic.
1. INTRODUCTION
A cervical abscess is a collection of pus in the cervical structures. It happens after a bacterial infection in the neck. Sometimes, a cervical abscess happens following an inflammation or infection of a congenital cervical mass. It’s a very rare disease in the neonatal period. The particularity of this article is the unusual occurrence of the cervical abscess in the newborn. We report two cases of deep neck abscess occurring in the Neonatology Intensive Care Unit (NICU) of Marrakech, Mohammed VI University Hospital, Marrakech (Morocco).
2. CASES REPORT
2.1. Case One
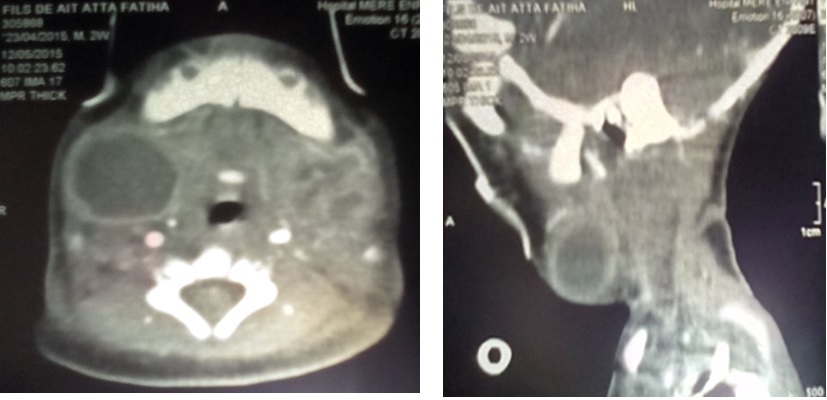
A two days old, male newborn, admitted in the NICU for seizures. The child was born vaginally at 38 weeks of gestational age. There were no incidents in the prenatal period or in the labor history. The physical examination and the capillary glycemia were normal. Initial laboratory tests revealed a White Blood Cells (WBC) count at 22970/mm3 with 14000/mm3 neutrophils, platelet count at 111000/mm3, the C reactive protein was normal (6.6mg/l), and a hypocalcemia of 75mg/l was found. The lumbar puncture, the blood culture and the cerebral function monitoring were normal. The transfontanellar ultrasound and the cerebral CT scan were normal. The hypocalcemia was treated by using intravenous calcium gluconate. After three days of his admission, the patient presented a nosocomial infection caused by Klebsiella Pneumonia resistant to 3rd generation Cephalosporin. We treated him with Imipenem and Amikacin for 10 days. After 9 days of treatment, we observed neck swelling (Fig. 1). The Ultrasonography revealed laterocervical cystic mass where cystic hygroma was suspected. A cervical CT scan was performed, revealing two bilateral laterocervical collections, related to an abscess (Fig. 2). The abscess puncture revealed pus, and Methicillin-Sensitive Staphylococcus Aureus (MSSA) was identified in this purulent material. The newborn was treated accordingly for ten days. An immune assessment was done including HIV serology and revealed no anomaly. After 23 days of hospitalization, the infant was discharged in good clinical evolution.

2.2. Case Two
A male newborn was admitted at four days of life for jaundice that appeared two days after his birth. The child was born by instrumental delivery (forceps). The Physical examination showed abrasion behind the left ear and peripheral facial palsy. Initial laboratory tests revealed: an anemia with a hemoglobin of 7.6 g/dl, the WBC was 10 000/mm3 with 5810/mm3 of neutrophils and the CRP was 142.2 mg/l, the total bilirubin was 135 mg/l (indirect 81 mg/l, direct 54 mg/l). Hemolytic causes were ruled out. Cytobacteriological urine exam showed a urinary infection to Klebsiella pneumonia treated with 3rd generation cephalosporin and gentamicin. The antibiogram confirmed the sensitivity of the germ. After 4 days of treatment, the patient became irritable, a limitation of the neck movement and bilateral neck swelling were observed (Figs. 3, 4). The Otomastoiditis was suspected first, and was ruled out after the CT scan showing a bilateral filling of the mastoid cells considered physiological in the newborn, there was no bone involvement. Hence, the swelling was localized where the forceps was performed. We concluded to an abcess and the diagnosis was confirmed after the punction revealing pus, but no isolate was identified in the pus or blood culture. An immune assessment was done including HIV serology and it was negative. The Treatment with 3rd generation Cephalosporin was continued during 14 days, after which the patient's clinical status improved, he completely recovered, the facial palsy caused by Forceps improved, and he was discharged home, the outcome was good.


3. DISCUSSION
We report two neck abscesses in the newborn, unusual in this period of life. The first was caused by MSSA, infection with favorably evolution on antibiotics and drainage. The second case is a post traumatic neck abscess caused by instrumental delivery (forceps) well managed, also treated using drainage and antibiotics. Many observations have been reported, concerning deep neck abcess in childhood [1]. However, it was rarely described in the neonatal period [1].The most pertinent researches in the English literature on cervical abscesses in the very young children were summarized by Oana Falup-Pecurariu et al. [2] and Mehmet Mutlu et al. [1]. The cervical abscess is more common in males in the neonatal period: the sex ratio is 2/1 [3]. Although in most cases, risk factors for neck abscess were absent, it is interesting to know that; some of the most common causes of cervical abscess were iatrogenic or congenital malformations [3]. In the cases reported, one of the patients had instrumental delivery which is probably the cause of his abscess. The most common symptoms at diagnosis were neck swelling, fever, dysphagia, breathing problems, irritability, bradycardia or tachycardia. Sometimes the cervical abscess may be afebrile [1]. The reported patients didn’t present fever; one of them presented irritability and limitation of neck movement. Neck swelling was noticed in one case after 13 days and in the other case after 4 days of hospitalization. Neck CT scan with contrast is currently the choice to diagnose neck abscess and complications, with a sensitivity of 94% [4]. In the second case the diagnosis was confirmed by clinical examination and by punction. Escherichia coli, S. aureus, and group B streptococcus are the most isolates identified in the neonatal deep neck abscesses [5]. In the second case no germs were found, probably explained by prior antibiotic. Due to the rarity of neonatal abscess occurrence, immune deficiency has to be ruled out as it was the case of these 2 patients. The treatment of choice of neck abscesses are antibiotics +/- associated to surgical drainage of the abscess [6]. The most serious complications in deep neck infections are mediastinal infections, paraplegia, vertebral osteomyelitis and compression of the airways [7-10]. The evolution in children with deep neck abscesses is good; this was the case in these two neonatal neck abscesses. Death in the neonatal period was reported by Coulthard and Isaac [11]
CONCLUSION
This report emphasizes the rarity of neonatal neck abscess, and the importance to ruling out the immune deficiency when the etiology is unknown.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this report.
CONSENT FOR PUBLICATION
A written informed consent was obtained from the parents.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

