
RESEARCH ARTICLE
Synthesis of Health Policies in the Fight against Malaria in Two Countries at Different Stages of Intervention in the Progress Towards Malaria Elimination, using Data from Surveys and Literature
Elvire Mfueni Bikundi1, *, Annie Robert2, Catherine Bouland3, Edouard Akotionga4, Ndèye Mareme Sougou5, Yves. Coppieters6
Article Information

Identifiers and Pagination:
Year: 2023Volume: 15
E-location ID: e187427932212260
Publisher ID: e187427932212260
DOI: 10.2174/18742793-v14-e221227-2022-2
Article History:
Received Date: 26/3/2022Revision Received Date: 27/9/2022
Acceptance Date: 3/11/2022
Electronic publication date: 07/04/2023
Collection year: 2023

open-access license: This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International Public License (CC-BY 4.0), a copy of which is available at: https://creativecommons.org/licenses/by/4.0/legalcode. This license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Aims:
The aim of our study was to provide a synthesis of successful policies applied in the fight against malaria in African countries at different stages of intervention; Burkina Faso and Senegal.
Background:
Malaria is a global public health problem with many cases each year in the world (241 million cases with 247,000 deaths; 67% were under five children) in 2020. Most malaria cases occur in Sub-Saharan African countries (93%).
Objective:
The objective of our study was to present policies implemented against malaria (with the best results) in these two African countries (Burkina Faso and Senegal) which are at different stages of intervention. These could serve as an example to others malaria endemics countries. To achieve our purpose, we used DHS survey data and information from a literature synthesis.
Methods:
Data used for analysis are from Demographics and Health Surveys (DHS) 2017-2018 for Burkina Faso and DHS 2017 for Senegal. We added information from a synthesis of the literature. Linear regression models were performed with an estimation of the mean number of persons using insecticide-treated nets among groups (urban or rural areas, wealth level, highest education level in the household and age of household head) in each country. We evaluated the importance of co-factors in the relationship between the number of ITNs in a household and the number of household members by calculating the R-squared.
A criteria grid used for this synthesis of literature included eight important sub-groups: funding sources, entomological monitoring, use of ITNs, use of insecticide, malaria case management, health system organization, communication and surveillance.
Results:
Senegal and Burkina Faso have the same proportion (51%) of households in which all children under 5 sleep under ITNs. We found R-squared (R2=0.007 in Burkina Faso and R2=0.16 in Senegal) for the relationship between the number of ITNs in a household and household size. When wealth level, age of head of household, area of residence (rural or urban), education level in the household and number of bedrooms in the household were controlled for, we found R2=0.106 for Burkina Faso and R2=0.167 for Senegal.
We found that Senegal’s National Malaria Program is decentralized with entomological monitoring in all districts, which is normal considering the intervention stage in the fight against malaria. In Burkina Faso, we found centralization of routine data.
Conclusion:
Our study synthesized the health policies applied in African countries which are at different stages of intervention in the fight against malaria and which have succeeded in maintaining low malaria prevalence (in Senegal) or in rapidly decreasing the prevalence of the disease (in Burkina Faso). Being close to elimination, Senegal required more active malaria surveillance than passive surveillance. Burkina Faso did not require a lot of active surveillance being not close to malaria elimination. These results encourage a review in the context of each African country.
1. BACKGROUND
Malaria is a global public health problem with many cases each year in the world (241 million cases with 247,000 deaths; 67% were under five children) in 2020. Most malaria cases occur in Sub-Saharan African countries (93%). The prevalence of malaria in some Sub-Saharan African countries is very high. While almost all African countries have set up a national program to fight malaria with grants from international organizations, local governments, and private funds, they have not made the same progress.
The question that would arise is what would be the best program to fight malaria in Sub-Saharan African countries? The successful and ideal program against malaria from which all countries can refer to fight against malaria does not exist. According to World Health Organization (WHO) recommendations for strategies to be adopted in the fight against malaria, there is no best model for fighting against malaria. Nevertheless, depending on each context and the targets recommended, each local context could have an adapted best program in the fight against malaria [1, 2].
Senegal and Burkina Faso are two West African countries, each of which has gross domestic products (GDP) of around 20 billion United States Dollars. Yearly minimum and maximum temperatures in Burkina Faso are 24.9 °c and 32.0°c, and in Senegal 24.5°c and 32.3°c. Yearly minimum and maximum rainfall in Burkina Faso are in millimeter (0.30 mm and 230.4 mm), in Senegal (0.18 mm and 261.36 mm). According to several studies carried out in Sub-Saharan African countries, malaria prevalence varies spatially, depending on several factors including socio-economic or environmental factors. It was found that poor’s households, urban areas, the quantity of precipitation, ITN use or other socio-economic or environmental factors are correlated to the increase in malaria risk. Senegal and Burkina Faso are at different stages of intervention in the fight against malaria regarding the progress towards elimination. Senegal is close to malaria elimination while Burkina Faso is not. The national malaria programs of both countries have been very successful in recent years. Senegal has maintained low malaria prevalence for several years and malaria cases number in Burkina Faso have decreased rapidly [3-5].
There have been good results from national malaria programs implemented in the last 10 years in these two African countries, despite the climate and socio-economic conditions, which are linked to high malaria risk. Several studies have found that the risk of malaria infection is influenced by climate (such as quantity of rainfall or air temperature) and by socio-economic factors (such as the economic status or education level of a family) which can influence some behaviors such as the use of nets [5-7].
According to the operational requirements for malaria elimination outlined by the World Health Organization, identifying and treating a high proportion of the population is crucial for countries that are not very close to elimination, they need to rapidly decrease malaria transmission. For countries that are close to malaria elimination, strengthening health systems with early detection and early treatment of malaria cases is critical for achieving malaria elimination [8].
Malaria is one of the major public health problems in Africa, with most cases and mortalities occurring among African children. Health policies in the fight against malaria have been implemented in Senegal and Burkina Faso, with good results in the reduction of national malaria prevalence. Studies have shown the importance of considering parameters such as funding, malaria case management, health information systems, collection of routine data for surveillance and other specific health policies in the assessment of malaria programs [9-11]. The aim of our study was to provide a synthesis of two different successful policies applied in the fight against malaria in African countries at different stages of intervention, Burkina Faso and Senegal. The synthesis of literature focused on differences between malaria programs implemented in the two countries which have had good results in the fight against malaria in the last ten years.
2. METHODOLOGY
2.1. Data
Using malaria diagnostic test results obtained from Demographics and Health Surveys (DHS), which are nationally representative surveys, we estimated malaria prevalence in each concerned country.
DHS data, used for quantitative analysis of ITN use, were from DHS 2017-2018 for Burkina Faso (malaria prevalence estimated with microscopy test was 17%) and from DHS 2017 for Senegal (malaria prevalence estimated with microscopy test was 1%). We used DHS data from 2010 to 2018 to estimate longitudinal progress concerning malaria prevalence in Burkina Faso and Senegal. Senegal (16 million inhabitants) is a west African country with a warm and tropical climate. The northern part of Senegal is very hot (dry Sahelian plain). Burkina Faso (20 million inhabitants) in the center of west Africa, is a landlocked Sahel country. The incidence of malaria in Burkina was 400 per 1,000 population at risk and in Senegal 400 per 1,000 population at risk, in 2018 (World Banque. Country Report) [3]. DHS survey is a cross-sectional, nationally representative survey carried out in developing countries. Firstly, each country was divided into small geographic areas (clusters) and in each cluster, three strata were created: towns, cities and rural or urban areas. In the second degree, households were selected (a two-stage sampling procedure) [2].
DHS surveys also collect socio-economic data, which we used in this study: urban or rural residence, economic level of the household, possession and use of an ITN, education level in the household, age of head of household, number of rooms in the house and number of household members. The construction of wealth quintiles is based on some considerations of the household population. Information such as water supply, type of vehicle, type of flooring, radio, television, refrigerator, electricity, domestic servants, ownership of agricultural land, sanitation facilities, or country-specific items was used for determining wealth level.
ITN ownership was measured with the number of ITNs in a household and ITN use was measured with the number of under five children number sleeping under ITN the night before the survey.
The prevalence of malaria was estimated using the population category of children aged 6-59 months in all selected households. During DHS surveys, a child infected with malaria was determined by several methods such as microscopy or rapid diagnostic test (RDT). For a rapid diagnostic test (RDT), the result of which, available after 15 minutes, was immediately communicated to the parents or persons responsible for the child. Positive cases received drugs considered to be first-line treatment in the country. To validate the results of the rapid malaria test, a microscopy test was performed. Blood smears were dried, fixed with methanol and packed. Results from microscopy testing were used for the present study [12].
We added information from a synthesis of official literature. The literature used was from the health ministries of each country and international authorities and agencies. We used methods proposed by Judith Green and Nicki Thorogood and we used a criteria grid. We selected official reports from 2010 to 2018, which accurately report national malaria programs in Senegal or Burkina Faso [13, 14]. The literature selected were WHO reports, President’s Malaria Initiative reports, United Nations Children’s Fund (UNICEF) reports [1, 12, 15, 16] and documents from the Ministries of Health of Senegal and Burkina Faso. The criteria grid used for this synthesis of the literature on malaria programs included eight important sub-groups: funding sources, entomological monitoring, use of ITNs, use of insecticide, malaria case management, health system organization, communication and surveillance.
2.2. Statistical Methods
Statistical analyses were performed using IBM SPSS version 20.0 and SAS studio. We performed a linear regression to investigate the relationship between the number of ITNs and the number of persons in a household, adjusted for the age of household head, the economic level of the household, the highest education level in the household and the area of residence (rural or urban). The normality and homoscedasticity of regression models were verified by observing the shape of points, curves in plots, and scatter plots of residuals. Figures representing R-squared in each model were shown with their confidence intervals at 95%.
We estimated the mean number of persons using ITNs among groups (urban or rural areas, wealth level, highest education level in the household and age of household head) and in each country using analysis of variance which is an important tool for multiple comparisons of groups.
The ANOVA provides much information, but it does not provide detailed information about differences between specific study groups. It was used to select a model that fits the best situation according to socio-economics factors [17].
We evaluated the importance of socio-economic factors in our linear regression model for the relationship between the number of ITNs in a household and the number of household members by computing the R-squared of each model. We must note that this evaluation was performed considering only areas of intermediate malaria endemicity (prevalence 5-40%) and high endemicity (prevalence >40%). Areas of low malaria endemicity (malaria prevalence <5) were not considered in this estimation.
Semi-partial correlation (correlated to R-squared) provides a solid estimate of the relative importance of each predictor in a multiple regression model. Studies have demonstrated the unique contribution of each independent variable in a multiple regression model. The square of semi-correlation represents how much the R-squared value decreases in a model when a predictor is removed. We used the decrease in the R2 value when a co-variable is dropped from the model to assess the importance of a factor in the model for each country (Senegal or Burkina Faso) [18].
3. RESULTS
Data from DHS surveys used are described in Table 1. We used a sample size of 6183 households for Burkina Faso and 12797 households for Senegal. Even if difference in sample size, each sample is a national representative for the concerning country.
We can observe that the proportion of the poorest households in Senegal (31.0%) is triple the proportion of the richest (8.8%). In Burkina Faso, there is almost the same proportion of all wealth levels in the population. The proportion of urban households in Senegal (34.1%) is double the proportion of urban households in Burkina Faso (15.8%). In 2010, malaria prevalence was 1% in Senegal and 66% in Burkina Faso (Fig. 1). Burkina Faso has made significant progress in decreasing malaria prevalence at the national level (from 66% in the year 2010 to 17% in the year 2018).
Fig. (1) Shows the longitudinal trend for malaria prevalence in these two countries (Senegal and Burkina Faso). We can observe that malaria prevalence in Burkina Faso has decreased greatly.
Studies found differences between the use and the ownership of ITN while the use of ITNs is an important element in the fight against malaria [19-21]. We compared the mean number of ITNs used in sub-groups for each country. We observed that the mean number of ITNs used is almost the same in urban and rural households in Burkina Faso with no significant difference (p-value=0.46). We found also that there is no significant difference in the number of ITNs used considering the highest education level in households in both countries (p-value=o.43 for Senegal and p-value=0.36 for Burkina Faso) (Table 2). Wealth level is an important factor in ITN use [21]. Poor households used significantly more ITNs than the richest households in both countries (Senegal and Burkina Faso), which is an effective policy. Studies have demonstrated that the poorest houses are at increased malaria risk due to the absence of windows with insect filters or other house qualities [22].
We found a positive linear relationship between the number of ITNs per household and the number of members per household in both countries. In Senegal and Burkina Faso, the number of ITNs per household increases with the household size (Fig. 2A and 2B). When we controlled the relationship between the number of ITNs and the number of household members with the age of household head, economic level of household, place of residence (urban/ rural), highest education level in the household and number of sleeping rooms in the household, we found for Burkina Faso (R2=0.106) and Senegal (R2=0.167) (Table 3).
| - | Burkina Faso | Senegal |
| Description of Countries** | ||
| Population (n) | 20,835,401 | 16,209,125 |
| Area in Km2 (% water body) | 274,400 (0%) | 196,722 (2.1%)* |
| Density (persons/km2) | 76 | 82 |
| Gross Domestic Products (USD/ persons) | 640 | 1033 |
| Human Development Index | 0.402 | 0.505 |
| Agriculture (% population) | 80 | 16 |
| Population below poverty line (%) | 33 | 33 |
| Gini index for income inequality | 35.3 (2014) | 40.3 (2011) |
| Description of DHS Data Used | ||
| Year of survey | 2017-2018 | 2017 |
| Sample size (N= number of households) | 6183 | 12797 |
| Proportion of urban population | 15.8% | 34.1% |
| Wealth level of households***: -Poorest -Poor -Middle -Richer -Richest |
20.5% 22.4% 20.5% 20.4% 16.2% |
31.0% 24.7% 22.4% 13.1% 8.8% |
| Malaria prevalence | 17.0% | 0.4% |
| Household where all under 5 children sleeping under ITN | 51.5% | 50.8% |
**: Data from World Bank [19] and from OECD (Organisation for Economic Co-operation and Development) [20].
***: Construction of wealth quintiles in DHS data is based on some considerations of household population. Information such as water supply, type of vehicle, type of flooring, radio, television, refrigerator, electricity, domestic servants, ownership of agricultural land, sanitation facilities, or country-specific items were used to determine wealth level.
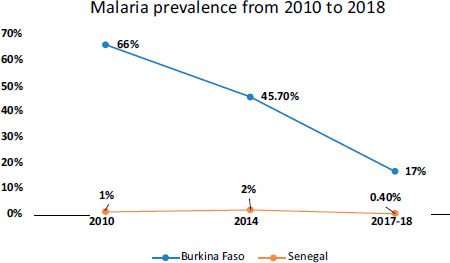 |
Fig. (1). Progress for malaria prevalence in Senegal and Burkina Faso from 2010 to 2018 (DHS surveys) [2]. |
| - | Senegal | Burkina Faso | ||||||
| Number of children who use ITNs in the household | Mean | Lower | Upper | P-value | Mean | Lower | Upper | P-value |
| Mean in -Urban areas -Rural areas |
1.20 1.38 |
1.13 1.32 |
1.33 1.42 |
0.002 | 0.96 0.99 |
0.88 0.95 |
1.04 1.03 |
0.46 |
| Mean by household economic level: -Poorest -Poor -Middle -Richer -Richest |
1.22 1.34 1.46 1.26 1.09 |
1.11 1.21 1.33 1.11 0.91 |
1.33 1.48 1.58 1.41 1.27 |
<0.0001 | 0.88 1.09 0.93 1.09 0.97 |
0.79 1.00 0.83 0.99 0.87 |
0.97 1.18 1.03 1.19 1.07 |
<0.0001 |
| Highest Education level in the household: -No education -Primary -Secondary -Higher |
1.28 1.28 1.39 1.17 |
1.21 1.15 1.22 0.72 |
1.35 1.41 1.55 1.62 |
0.43 | 0.98 1.06 0.97 0.88 |
0.93 0.941 0.85 0.43 |
1.03 1.18 1.08 1.33 |
0.36 |
| Age of head of household: -Under 25 -25 to 50 years - Over 50 years |
1.14 1.20 1.63 |
0.90 1.14 1.51 |
1.39 1.27 1.75 |
<0.0001 | 0.81 1.00 1.03 |
0.68 0.96 0.90 |
0.94 0.96 0.90 |
0.003 |
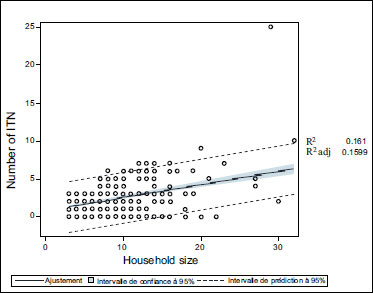 |
Fig. (2A). Evolution of ITN number according to number of household members in Senegal. |
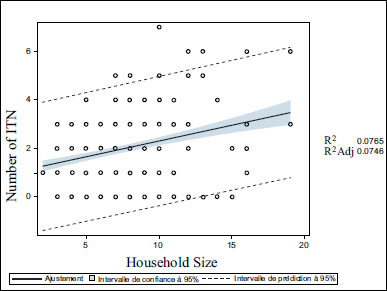 |
Fig. (2B). Evolution of ITN number according to number of household members in Burkina Faso. |
This result indicates that in Senegal, the number of ITNs in a household increases more rapidly with the size of the household than in Burkina Faso. Senegal needs to do more than apply the universal distribution of ITNs. If a resurgence of the disease is to be avoided, Senegal must also organize free distribution in targeted areas and to targeted sub-groups according to surveillance data.
We observed that socio-economic and demographic factors such as the age of household head, economic level of household, place of residence (urban/ rural), highest education level in the household, and number of sleeping rooms in the household had almost the same effect on the possession of ITNs in Senegal, with the place of residence (urban or rural) having a slightly greater effect than other factors. In Burkina Faso, the wealth level of households had a little more influence than other socio-economic factors on ITN possession (Table 4).
Socio-economic factors such as wealth level must be overcome by policies implemented against malaria. Several studies have noted that poor households have a greater need for the use of ITNs than the richest households [23]. It is very important to reach all categories of households for the distribution of ITNs, particularly households in targeted areas.
Table 4 provides a synthesis of the policies implemented against malaria in both countries. We can observe that a lot of active surveillance and control such as home-based tests and treatments have been conducted in Senegal, compared to home-based tests and treatments in Burkina Faso [8].
4. DISCUSSION
The objective of our study was to synthesize policies implemented against malaria (with the best results) in these two African countries (Burkina Faso and Senegal), which are at different stages of intervention, but the objective was not to compare the two countries. The goal was to show two different models of malaria control that give good results. To achieve our purpose, we used DHS survey data and information from a literature synthesis. National representative surveys which include data on diagnostic malaria tests showed that the prevalence of malaria differs greatly from one African country to another. Significant differences in the prevalence of malaria are found even between neighbouring countries. In the last 10 last years, national malaria prevalence in Burkina Faso has significantly decreased and malaria prevalence in Senegal has remained very low (around 1%) for several years.
| Model | R2 of model | |
| Burkina Faso | Senegal | |
| Model with all variables | 0.106 | 0.167 |
| Model without age of household head | 0.105 | 0.167 |
| Model without wealth level of household | 0.096 | 0.166 |
| Model without place of residence (Urban/ rural) | 0.105 | 0.163 |
| Model without highest education level in the household | 0.104 | 0.167 |
| Model without number of sleeping room in household | 0.098 | 0.165 |
| Politics |
Countries Senegal Burkina Faso |
|
|
Funding |
Around $ 20,000,000 of external funds per year. Some main Donors: US National Institute of Health, UK Department for International Development, European Commission, Wellcomtrust, Bill and Melinda Gates Foundation, France, WHO, Usaid/Pmi, others. |
Around $ 25,000,000 of external funds per year. Some main Donors: US National Institute of Health, UK Department for International Development, European Commission, Wellcomtrust, Bill and Melinda Gates Foundation, WHO, Usaid/Pmi, others. |
|
Entomological Monitoring |
In each district during rainy season research on: resistance testing, species composition, feeding preferences, sporozoite rates. | In some districts: annual entomological monitoring.as Solenzo, Kampti |
|
Use of ITNs 1. Mass distribution 2. Routine distribution |
-Free distribution of 1.8 per person every three years. -For pregnant women, free distribution of ITNs (from first antenatal consultation). -For children, free distribution once a year (in targeted regions). |
-Free distribution of 1.8 per person every three years. -For pregnant women, free distribution of ITNs (not always to all pregnant woman. -Free distribution of ITN during immunization program. |
|
Insecticide Use 1. Indoor residual spraying 2. Insecticide resistance management |
Indoor residual spraying in a whole district where malaria incidence is more than 50 per 1,000 persons and where indoor biting is most common. Studies have been performed on the acceptability of this procedure. This is an acceptable intervention that has been proven to work. Resistance tests were performed for several insecticides in different districts. |
Policy not yet implemented. Resistance tests were performed for insecticides in some districts. Insecticide resistance studies have been done in Burkina Faso and this has enabled the malaria program to order the new generation mosquito nets for the distribution campaign that took place in 2019. |
|
Malaria Cases Management 1. Diagnosis 2. Treatment |
-In high transmission areas, once a week during rainy season, health workers experiencing fever took a home-based test. Treatment was provided to positive cases. This also applied to children under the age of 5 years. -In areas with less than 5 cases per 1,000 persons, investigations in patient’s household. -First line treatment is Artesunate-Amodiaquine, Artemether-Lumefantrine, Dihydroartemisinin-piperaquine. -Seasonal malaria chemoprevention is implemented in some regions according to WHO recommendations. -Availability of malaria commodities because of better management due to: training of health workers (best prescribing) and use of drug management software (SAGE) in the health system information. |
-RDT is used for almost all malaria diagnostic testing. Microscopy is used to confirm malaria cases (in health facilities). The confirmation rate was 77.5% in 2014, 91.7% in 2017 and 97.6% in 2018. -First line treatment is Artesunate-Amodiaquine, Artemether-Lumefantrine, (10,457,752 cases in 2017 and 10,807,674 cases in 2018 treated with ACT, and 281,535 in 2017 and 267,194 cases in 2018 of treated with injectable artesunate). -Chemoprevention during peak season with Artesunate-Amodiaquine for children under five. -Several training courses on malaria case management for health workers. |
| Health System | -Introduction of malariology course in nursing training. -Several training courses for managers, health workers in hospitals and in laboratories: performance-based financing for producing high impact health budget for a specific country, training on case management and diagnosis at hospital and at home, quality control of drugs (register of drug equivalence). This program is supported by the university and the PNLP*. Malaria diploma is credited by UCAD**. -Research for new intervention: research policy concerning feasibility of intervention and their acceptability. -Conduction of integrated logistic visits in all regions for delivering a detailed report. -Audits are frequently performed. -Decentralization of malaria program implementation. As an example, the management of promotional and prevention activities is done according to the local context of each community. |
-Yearly training courses for malaria program staff and for all health workers. -Elevation of Burkina Faso Malaria National Program in the organigram of Ministry of Health for more efficiency and direct interaction. -Implementation of drug efficacy studies. - The removal of barriers to geographic and financial accessibility through investments and the implementation of subsidy and free policies (peaks from 2016) have contributed to better attendance by populations at health facilities and to better notification of cases. Hence, the increase in prevalence and / or incidence. However, cases of severe malaria and its lethality have decreased significantly due to the fact that the population has easy access to consultation and receives good quality care. At the central level: The planning of malaria control activities revolves around the development of five-year strategic plans. Funding and management of the malaria control program is done at the federal level. |
| Communication | -Mass communication: during theater, with radio communication, home visits (local context is considered). | -Mass communication campaign: education of population by film projection, theater, home visits. |
| Surveillance | -Annually, continuous Demographic Health survey. -Centralization of all relevant malaria data from health posts in each district (creation of a web-platform). |
-Collection of routine data from: district health centers, surveys (DHS, MIS) and data from surveillance sites. Some demographic and health surveillance sites are already functional ( Nouna, Sapone and Kaya). |
UCAD**: University Cheikh Anta Diop de Dakar (Senegal).
References for Synthesis of literature: [1, 12, 15-16, 24-36]
4.1. Funding
Like almost all African countries, Senegal and Burkina Faso have national malaria programs supported by international and other external funds [32-35]. Most of the funding for the fight against malaria in both countries comes from international partners such as the United State National Institute of Health, the United Kingdom Department for International Development, the European Commission, the Wellcomtrust and the Bill and Melinda Gates Foundation.
The big question is whether those external funds are adequately distributed according to the needs of the national malaria programs in Burkina Faso and Senegal [33, 35]. Head, who investigated malaria research funds in African countries from 1997 to 2015, found that Burkina Faso is in the group of the highest-funded African countries concerning research on malaria (more than $ 30 million) and Senegal is in the second highest-funded group of countries ($ 5-30 million) [36].
It is crucial that the use of funds responds to the real needs of a country. A study by Barrenho demonstrated the importance of effective coordination among different donors of malaria funds if a good level of performance in relevant policies is to be achieved [37].
4.2. Entomological Monitoring
Entomological research is an important part of research for implementing regional policies against malaria. In Senegal, entomological monitoring is conducted several times a year in each district [22] and in Burkina Faso, it is conducted once a year in some districts. This does not necessarily indicate that one country’s entomological monitoring is more effective than the others. It can be a difference in strategy based on the country's context and stage of intervention in the fight against malaria. Burkina Faso may have a few highly relevant sentinel sites, a system that can be as effective as covering each district. As malaria has almost been eliminated in Senegal, a lot of active surveillance and control, including vector surveillance, is necessary. It is important for Senegal to have an entomological surveillance site in each district, but it is not necessary for Burkina Faso if fewer sentinel sites can adequately cover the whole country. Studies have found that several changes occur in mosquito behavior, mosquito abundance, composition, and dominant vectors, sometimes due to policies implemented in the fight against malaria such as the use of ITNs, the use of insecticide, or chemoprevention. Entomological monitoring is an important element in the initial stages of the implementation of a malaria intervention policy and for surveillance [38].
4.3. ITN Policy
Both countries have applied a policy of free distribution of ITNs (1.8 ITNs per person every 3 years) throughout the population. Senegal does more with the additional free distribution of ITNs every year in targeted districts and to targeted populations, such as children under five.
Knowing that Burkina Faso is more populated than Senegal and the proportion of the poorest households in Senegal (31.0%) is triple the proportion of the richest in Burkina Faso (8.8%), this is particularly important for household ownership of bed nets and use. It must be noted also that wealthy people may have access to good housing, good sanitation and environmental management, aid conditioner, etc. All factors are determinants to be considered when providing interpretation. Quantitative data used in this paper is about the possession of ITN and the use of ITN. Senegal and Burkina Faso have the same proportion (51%) of households in which all children under 5 sleep under an ITN. In general, the wealth level of households has a positive relation with ITN possession but a negative relation with ITN use. This must be considered in the management of the fight against malaria. As mentioned before, although studies have demonstrated that the poorest houses are potentially at higher malaria risk than the richest houses, this should be relatively discussed with the fact that wealthy people have more access to a clean environment, access to other means of protection from malaria and may not need necessary bed nets compared to the poorest household. In Senegal, there is a significant difference between the mean number of ITNs owner in households in rural and urban areas, but in Burkina Faso, there is no significant difference. A study by Thwing explained that the difference between ITN numbers in urban and rural households in Senegal was due to the fact that Senegal also applied free ITN distribution to children under five. As rural households had more children under five than urban households, it was logical that there were more ITNs in rural areas than in urban areas in Senegal [39].
For both countries, in rural areas, there is a little more use of mosquito nets than in urban areas (not a significant difference). Due to suitable environments for mosquito breeding sites, malaria is mainly transmitted in rural areas and can influence the use of ITN. The study of Mfueni found that there is more risk of malaria in rural areas than in urban areas [5].
Several studies have demonstrated that the use of ITNs can greatly reduce malaria risk by reducing the rate of mosquito bites and the density of mosquitoes [23]. Wealth level is an important factor in ITN possession in African countries [30]. We found that poor households had the highest mean number of ITN use in both Senegal and Burkina Faso. Studies have demonstrated that the poorest houses are potentially at higher malaria risk than the richest houses [31].
The possession of ITNs does not necessarily equate to the use of ITNs. The use of ITNs in a population is strongly associated with the education of the population on the prevention of malaria. Senegal and Burkina Faso have implemented communication policies appropriate for the local context and level of education. We found that in Senegal and Burkina Faso, there is no significant difference in the use of ITNs in relation to the highest education level in the household. The wealth level of households is the most important factor for ITN possession in Burkina Faso (R2=0.096) but not in Senegal (R2=0.166) for the model of the relationship between ITN possession with some socio-demographic factors as shown in Table 3.
4.4. Insecticide Use
Resistance tests for insecticide are performed in Senegal and Burkina Faso. A policy of indoor residual spraying has not been applied in Burkina Faso, whereas Senegal has implemented indoor residual spraying in districts where the incidence of malaria is higher than 50 per 1,000 persons. Studies have demonstrated the effectiveness of indoor spraying in the fight against malaria. A study by Pluess using randomized comparison found that indoor residual spraying significantly reduces the prevalence of malaria in unstable settings [40, 41]. In Senegal, there has been a reduction of immunity in the population. The risk of a rapid resurgence is therefore highly possible if all areas are not under control. A policy of indoor spraying is an effective tool for rapidly decreasing mosquito vector capacity in targeted areas. It must be noted that the use of ITNs in both countries has also contributed to a decrease in vector capacity.
Insecticide resistance research is being conducted in the two countries to determine which insecticide can be used against local malaria vectors. The study of insecticide resistance in the fight against malaria is very important and can influence malaria control in several ways. Resistance to insecticide may produce a gap between the entomological studies and the efficacy of epidemiological studies [24].
4.5. Case Management
First line treatment is the same in the two countries, but we found a great difference between Senegal and Burkina Faso concerning the diagnosis of cases. As malaria has almost been eliminated in Senegal, more targeted case management in high-transmission areas is necessary. Home-based diagnosis is performed and health workers with the objective of rapidly decreasing malaria transmission give malaria treatment to positive cases. Senegal introduced home-based management of malaria cases in 2008 with rapid diagnostic tests and artemisinin-based combination therapy as a treatment for positive cases [42].
A study by Landier demonstrated the importance of early diagnosis and treatment in the reduction of malaria transmission. In the case of P. falciparum malaria cases, treatment within 48 hours from the onset of fever is a preventative action against malaria transmission. Without early diagnosis and treatment or with the incomplete treatment of victims following bites from infected mosquitoes, gametocyte remains in those individuals for several days after clearance of asexual parasites. They remain infected and can transmit malaria [25].
4.6. Health System Organization
Senegal’s national malaria program is decentralized, but the opposite is the case in Burkina Faso. A centralized program is a system in which the federal government makes the decision for all areas in the country. Decentralization allows Senegal to implement a more effective malaria program according to the context of each district, considering, for example, dominant vector species, the quantity of rainfall and temperature, and the education level of the population. As a country close to eliminating malaria, Senegal must closely monitor all districts to avoid a resurgence of the disease and maintain very low transmission. A study published in 2016 demonstrated the benefits of local contextualization of policies implemented in the fight against malaria [43].
4.7. Communication Policy
Local context is more widely used in communication policies for the national malaria program of Senegal and Burkina Faso. The most appropriate methods of communication for reaching a targeted population must be tailored for different regions. The culture of each region or its socio-economic conditions must be considered if the best results are to be achieved from malaria programs [44]. In Senegal, research policies on the feasibility of interventions and their acceptability are integrated into the national malaria program [28-31]. Several studies converge, finding that it is better to work within a local than a national context to eliminate this significant public health problem in Africa.
4.8. Surveillance
In Senegal, a demographic and health survey with epidemiological centers for surveillance in each district is organized every year. In Burkina Faso, routine data are collected from all districts and data from surveys (questionnaires) by mobile phone. We can observe that malaria surveillance implemented in Burkina Faso is more passive than active, while in Senegal (a country close to malaria elimination), malaria surveillance is more active than passive. Active surveillance contributes to the reduction of malaria transmission and will facilitate malaria elimination. Testing and treating during active surveillance enable the identification of people who do not go to hospitals and facilitates the early detection of malaria cases, which reduces malaria transmission. A study by Singh found that active surveillance is an effective element in policies implemented for malaria elimination [45].
4.9. Limitations and Merits
Although the strength of our study was to combine information from a synthesis of the literature with quantitative data, there are some limitations. Due to the unavailability of data in the two countries, the quantitative analysis only focused on the relationships between the number or use of ITNs with the number of people in a household (with socioeconomic and demographic factors controlled for). Therefore, the results of the analysis show and focus only on the vector interventions while information on other policies was collected during DHS surveys but is not available. The results of this study highlight the ITN net interventions with the correlation to household size. It is the partial segment of the malaria control (elimination) policy that cannot conclude all other confounding factors related to malaria. It lacks, for example, additional quantitative analyses of the availability and quality of diagnostic tests, treatment and other interventions. We hope that future studies can address this limitation. Considering that the prevalence of malaria and the use of ITNs were estimated on children under five years old, it is necessary to take a step back and consider confounding elements between the wealth level of households and the use of ITNs (number of children in the household, rural/ urban areas, quality of housing, number of rooms). We would like to use more demographic factors in our models. Another demographic information associated with the household in our DHS data was the sex of the head of the household (apart from the age of the head of the household). We did not use the sex of the head of the household in our statistical models because almost all the households involved in the data used had male household heads.
CONCLUSION
We synthesized health policies implemented in the national malaria programs of Senegal and Burkina Faso considering a criteria grid with the policy on entomological monitoring, the use of ITNs, the use of insecticides, management of malaria cases, health system organization, communication and surveillance, highlighting our synthesis on some differences in these two National malaria programs. Knowing that comparison between the two countries was not the purpose of our study, a systemic conclusion will not be given because few details do not matter in descriptions of policies implemented in the two countries or on transmission information.
From 2010 to 2018 malaria prevalence in Senegal remains almost the same (around 1%) and in Burkina Faso, malaria prevalence decreased greatly (66% to 17%). We found that wealth level remains an important factor for ITN use in both countries; the poorest households use more ITN than the richest households. It can be due to the qualities of households or the use of insecticide. We found for Burkina Faso (R2=0.106) and Senegal (R2=0.167), the relationship between the number of ITNs and the number of household members, controlled by the age of household head, economic level of household, place of residence (urban/ rural), highest education level in the household and number of sleeping rooms in the household; what means more variance in Burkina Faso than in Senegal for ITN ownership. In Senegal, entomological monitoring is conducted in each district and in Burkina Faso, it is conducted in some districts once a year. In Senegal, health workers carry out weekly home tests in areas of high transmission during the rainy season for under five children, which is not necessary for Burkina Faso. Artesunate-Amodiaquine is one of the first-line treatment for malaria in Senegal and Burkina Faso.
As malaria has almost been eliminated in Senegal, a lot of active monitoring and surveillance is necessary, such as entomological monitoring in each district or an indoor residual spraying policy, in order to rapidly and locally decrease mosquito vector capacity. Senegal’s national malaria program is decentralized and the opposite is the case in Burkina Faso. However, we found the centralization of routine data in Burkina Faso to be effective. Being close to malaria elimination and having neighboring countries with high malaria transmission areas, it is challenging for Senegal to maintain a stable low transmission level, particularly as the immunity of its population against malaria is decreasing [46].
The health systems of countries close to malaria elimination must be strengthened by robust research, particularly on factors that have a significant impact on transmission. These countries must be able to swiftly detect an increase in malaria cases in all areas. To maintain control of this low malaria transmission, Senegal needs to conduct entomological research in all areas to determine vector capacity in each district (longevity, density and bionomics of the mosquitoes prevalent in the concerned areas) and to improve health systems. This monitoring in all areas will enable more active surveillance for malaria case management within specific local contexts. If malaria is to be eliminated, the national malaria prevalence in Burkina Faso must be reduced. The malaria program of Burkina Faso must decrease the malaria reproduction rate to a rate lower than one. Implemented health policies must rapidly reduce mosquito vector capacity and human infectivity to rapidly decrease the malaria reproduction rate. Mosquito capacity as a malaria vector can be reduced through IRS (which influences the daily survival rate) and the use of ITNs (which influences the daily survival rate and human biting rate). Human infectivity can be reduced through early and effective malaria treatment [46].
Data used in our study confirmed what the synthesis of the literature demonstrated. Due to data availability, only the ITN policy has been analysed while the other policies are only described. The mean number of ITNs used per household in Burkina Faso is almost the same as in Senegal. The importance of the combination of all policies applied in accordance with the local context and the stage of malaria intervention was indicated. As malaria has almost been eliminated in Senegal, more active malaria surveillance than passive was necessary. In Burkina Faso, which is not close to malaria elimination, a lot of active surveillance was not necessary to decrease malaria prevalence in the country. A study by Gachelin et al. demonstrated the importance of combining strategies with various policies against malaria to achieve a better result [47].
Even if they do not have the same interventions in the fight against malaria, these two countries are examples of successfully implemented health policies. The incidence of malaria in Senegal remains low for several years and the incidence of malaria decrease exponentially in Burkina Faso over these last ten years. Senegal has achieved a lot in terms of reducing malaria prevalence. Such experience should be suggested for Burkina Faso in terms of starting to implement gradual demographic and health surveys with epidemiological centers. In Burkina Faso, some demographic and health surveillance sites are already functional. These could serve as an example to include a package of intervention and gradually more additional districts. In addition, in terms of policy implication, it is important to recommend more decentralization of malaria fights across health system levels for more effectiveness. We believe that decentralization including community involvement is key to reducing the malaria burden. A centralized system is very often proved to be less efficient. Although active case detection is recommended for the country having reached the elimination stage. Regarding this paper, we can also recommend mass treatment in highly affected areas in complement to chemoprevention already conducted in some Burkina Faso districts [47].
Considering the level of the fight against malaria, and economic or political choices, the strategies can be different and adapted. In countries close to malaria elimination, active policies more than passive policies are essential to keep the prevalence of malaria very low, such as continuous entomological surveillance and in all areas or early diagnosis. The purpose of this study was not to demonstrate the difference in the policies applied in the fight against malaria, but the purpose of this study was to demonstrate that whatever the reason that a strategy is adopted in the fight against malaria if it is done considering local context, it can lead to good results.
Our study provided a synthesis of the health policies applied in African countries at different stages of intervention in the fight against malaria, which has strongly succeeded in maintaining low malaria prevalence (in Senegal) or in rapidly reducing it (in Burkina Faso). These results merit a review in the context of each African country. We observe that there is no best model for fighting against malaria, but each national program can be the best if it considers the local context.
LIST OF ABBREVIATIONS
| GDPs | = Gross domestic products |
| PNLP | = National fight program against malaria (in French). |
| UCAD | = University Cheikh Anta Diop de Dakar (Senegal) |
| ITNs | = insecticide-treated net |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
The authors confirm that written informed consent has been taken for the collected data through a survey, in compliance with good practices.
STANDARDS OF REPORTING
STROBE guidelines were followed.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the (Demographic and Health Survey) at (https://dhsprogram.com/data/), reference number [2].
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
REFERENCES
| [1] | World Health Organization. World Malaria Report 2021. Available from: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2021 |
| [2] | Demographic and Health Survey. Surveys Data (2000-2018). Available from: https://dhsprogram.com/Data/ |
| [3] | World Banque. Country Report (2000-2018). Available from: https://data.worldbank.org/country |
| [4] | WorldClim. Global Climate Data2000. Available from: https://www.worldclim.org/ |
| [5] | Mfueni Bikundi E, Coppieters Y. Importance of risk factors associated with malaria for Sub-Saharan African children. Int J Environ Health Res 2017; 27(5): 394-408. |
| [6] | Tusting LS, Bottomley C, Gibson H, et al. Housing improvements and malaria risk in Sub-Saharan Africa: A multi-country analysis of survey data. PLoS Med 2017; 14(2): e1002234. |
| [7] | Diallo A, Sié A, Sirima S, et al. An epidemiological study to assess Plasmodium falciparum parasite prevalence and malaria control measures in Burkina Faso and Senegal. Malar J 2017; 16(1): 63. |
| [8] | World Health Organization. From malaria control to malaria elimination 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/112485/9789241507028_eng.pdf?sequence=1 |
| [9] | Lechthaler F, Matthys B, Lechthaler-Felber G, et al. Trends in reported malaria cases and the effects of malaria control in the Democratic Republic of the Congo. PLoS One 2019; 14(7): e0219853. |
| [10] | Ashton RA, Bennett A, Yukich J, Bhattarai A, Keating J, Eisele TP. Methodological considerations for use of routine health information system data to evaluate malaria program impact in an era of declining malaria transmission. Am J Trop Med Hyg 2017; 97(3_Suppl): 46-57. |
| [11] | Scott N, Hussain SA, Martin-Hughes R, et al. Maximizing the impact of malaria funding through allocative efficiency: using the right interventions in the right locations. Malar J 2017; 16(1): 368. |
| [12] | DHS, MEASURE. Household Survey Indicators for Malaria Control. 2013. Available from: tion.org/resources/publications/ms-13-78 |
| [13] | Green Judith, Thorogood Nicki. Qualitative Methods for Health Research. 1 Oliver’s Yard 55 City Road London EC1Y 1SP: SAGE Publications Ltd. 2004. |
| [14] | Aitken S. UNICEF Innocenti Research Centre. ‘Literature Review on Qualitative Methods and Standards for Engaging and Studying Independent Children in the Developing World. 2009. Available from: https://www.unicef.org/ |
| [15] | President’s Malaria Initiative. National Report 2018. Available from: https://www.pmi.gov/about |
| [16] | UNICEF. United Nation International Children’s Emergency Fund Available from: https://www.unicef.org/ |
| [17] | McHugh ML. Multiple comparison analysis testing in ANOVA. Biochem Med (Zagreb) 2011; 21(3): 203-9. |
| [18] | Liu J, Lou L, Li R. Variable selection for partially linear models via partial correlation. J Multivariate Anal 2018; 167: 418-34. |
| [19] | World Bank. 2020. Available from: https://data.worldbank.org/country |
| [20] | Organisation for Economic Co-operation and Development. 2020. Available from: https://www.oecd.org/about/members-and-partners/ |
| [21] | Rudasingwa G, Cho SI. Determinants of the persistence of malaria in Rwanda. Malar J 2020; 19(1): 36. |
| [22] | Govella NJ, Chaki PP, Killeen GF. Entomological surveillance of behavioural resilience and resistance in residual malaria vector populations. Malar J 2013; 12(1): 124. |
| [23] | Wanzirah H, Tusting LS, Arinaitwe E, et al. Mind the gap: house structure and the risk of malaria in Uganda. PLoS One 2015; 10(1): e0117396. |
| [24] | Snyman K, Bigira V, Greenhouse B, et al. Poor housing construction associated with increased malaria incidence in a cohort of young Ugandan children. Am J Trop Med Hyg 2015; 92(6): 1207-13. |
| [25] | Landier J, Parker DM, Thu AM, et al. The role of early detection and treatment in malaria elimination. Malar J 2016; 15(1): 363. |
| [26] | Kleinschmidt I, Bradley J, Knox TB, et al. Implications of insecticide resistance for malaria vector control with long-lasting insecticidal nets: a WHO-coordinated, prospective, international, observational cohort study. Lancet Infect Dis 2018; 18(6): 640-9. |
| [27] | Ministry of Health of Senegal. National Malaria Control Strategic Plan. Available from: http://www.pnlp.sn/wp-content/uploads/2016/08/PNLP_PSN_VFF_03-02-2016.pdf |
| [28] | Sy O, Cisse B, Tairou F, et al. Étude de l’acceptabilité de l’aspersion intradomiciliaire d’insecticide à effet rémanent dans le centre-ouest du Sénégal. Bull Soc Pathol Exot 2015; 108(3): 213-7. |
| [29] | Cissé B, Ba EH, Sokhna C, et al. Effectiveness of Seasonal Malaria Chemoprevention in Children under Ten Years of Age in Senegal: A Stepped-Wedge Cluster-Randomised Trial. PLoS Med 2016; 13(11): e1002175. |
| [30] | Tine RCK, Ndiaye P, Ndour CT, et al. Acceptability by community health workers in Senegal of combining community case management of malaria and seasonal malaria chemoprevention. Malar J 2013; 12(1): 467. |
| [31] | Tine RCK, Ndour CT, Faye B, et al. Feasibility, safety and effectiveness of combining home based malaria management and seasonal malaria chemoprevention in children less than 10 years in Senegal: a cluster-randomised trial. Trans R Soc Trop Med Hyg 2014; 108(1): 13-21. |
| [32] | Ministry of Economy, Finance and Development of Burkina Faso. National Institute of Statistics and Demography. National Institute of Statistics and Demography Burkina Faso: Malaria Indicator Survey (EIPBF) (2017-2018). Available from: http://www.insd.bf/n/contenu/enquetes_recensements/enquete_palu/EIPBF_2018.pdf |
| [33] | Burkina Faso Ministry of Health. Health accounts (2010-2018). Available from: https://www.sante.gov.bf/ressources/documents |
| [34] | Namountougou M, Simard F, Baldet T, et al. Multiple insecticide resistance in Anopheles gambiae s.l. populations from Burkina Faso, West Africa. PLoS One 2012; 7(11): e48412. |
| [35] | Ministry of Economy, Finance and Development of Burkina Faso. National Institute of Statistics and Demography. Burkina Faso Ministry of Health Statistical Yearbooks (2018). 2018. Available from: http://www.insd.bf/n/contenu/pub_periodiques/annuaires_stat/Annuaires_stat_nationaux_BF/Annuaire_Statistique_National_2018.pdf |
| [36] | Head MG, Goss S, Gelister Y, et al. Global funding trends for malaria research in sub-Saharan Africa: a systematic analysis. Lancet Glob Health 2017; 5(8): e772-81. |
| [37] | Barrenho E, Miraldo M, Shaikh M, Atun R. Vertical and horizontal equity of funding for malaria control: a global multisource funding analysis for 2006–2010. BMJ Glob Health 2017; 2(4): e000496. |
| [38] | Gatton ML, Chitnis N, Churcher T, et al. The importance of mosquito behavioural adaptations to malaria control in Africa. Evolution 2013; 67(4): 1218-30. |
| [39] | Thwing JI, Perry RT, Townes DA, Diouf MB, Ndiaye S, Thior M. Success of Senegal’s first nationwide distribution of long-lasting insecticide-treated nets to children under five - contribution toward universal coverage. Malar J 2011; 10(1): 86. |
| [40] | Alout H, Roche B, Dabiré RK, Cohuet A. Consequences of insecticide resistance on malaria transmission. PLoS Pathog 2017; 13(9): e1006499. |
| [41] | Pluess B, Tanser FC, Lengeler C, Sharp BL. Indoor residual spraying for preventing malaria. Cochrane Libr 2010; 2010(4): CD006657. |
| [42] | Gaye S, Kibler J, Ndiaye JL, et al. Proactive community case management in Senegal 2014–2016: a case study in maximizing the impact of community case management of malaria. Malar J 2020; 19(1): 166. |
| [43] | Murhandarwati EEH, Fuad A, Sulistyawati , et al. Change of strategy is required for malaria elimination: a case study in Purworejo District, Central Java Province, Indonesia. Malar J 2015; 14(1): 318. |
| [44] | Essé C, Utzinger J, Tschannen AB, et al. Social and cultural aspects of ‘malaria’ and its control in central Côte d’Ivoire. Malar J 2008; 7(1): 224. |
| [45] | Singh N, Bharti PK, Kumre NS. Active v. passive surveillance for malaria in remote tribal belt of Central India: Implications for malaria elimination. Pathog Glob Health 2016; 110(4-5): 178-84. |
| [46] | Mendis K, Rietveld A, Warsame M, Bosman A, Greenwood B, Wernsdorfer WH. From malaria control to eradication: The WHO perspective. Trop Med Int Health 2009; 14(7): 802-9. |
| [47] | Gachelin G, Garner P, Ferroni E, Verhave JP, Opinel A. Evidence and strategies for malaria prevention and control: a historical analysis. Malar J 2018; 17(1): 96. |





