All published articles of this journal are available on ScienceDirect.

Pott’s Disease in a 3 Years Old Italian Child: Case Report and Review of the Literature
Authors Info & Affiliations
Abstract
Introduction:
Tuberculosis (TB) is currently a major health problem, in particular in developing countries and in HIV positive people. Tubercular spondylodiscitis is the most common type of skeletal TB, more frequent in children than adults. It is rarely reported in developed countries.
Case Report:
We describe a 3 years-old Italian girl who referred to our hospital with back pain and walking deficiency; she had a very good outcome with anti-tubercular treatment and orthopedic follow-up.
Conclusion:
Early recognition and treatment of this tubercular complication are very important due to its possible complications: bone destruction, spinal deformity, neurologic and orthopedic complications.
1. INTRODUCTION
Tuberculosis (TB) is a common worldwide disease caused by the Gram-negative bacteria Mycobacterium tuberculosis. The World Health Organization (WHO) estimated a global TB incidence of 10.4 million of new cases during 2016, mostly coming from the WHO South-East Asia Regions (45%), the WHO African Regions (25%) and the WHO Western Pacific Region (17%). The top five countries for TB were (in descending order) India, Indonesia, China, the Philippines and Pakistan. TB is also reported with more frequency in males and HIV positive patients [1].
Tubercular spondylodiscitis (Pott’s Disease) is an extra-pulmonary manifestation of TB, characterized from the hematological dissemination of the infection to the spine. It was described for the first time in 1779 by Percivall Pott [2], and actually represents the most common form of skeletal TB, in particular in children [3-5]. This manifestation can lead to bone destruction, spinal deformity, neurologic and orthopedic complications.
Signs and symptoms of Pott’s disease are generally non-specific and characterized by back pain, intermittent fever, anorexia, night sweat, weight loss and paraparesis, with a very low progression.
The diagnosis is clinical and radiological in countries with a high TB prevalence, but it is very difficult to recognize in backgrounds where the disease is not endemic. An early diagnosis and an immediate anti-tubercular treatment are essential to improve the outcome [5]: spinal tuberculosis can lead to kyphotic deformity and orthopedic/neurological sequelae [6], and a specialist follow-up is required in these patients.
2. CASE REPORT
A 3 years-old Italian girl referred to our accident and emergency department on Saturday afternoon with a history of intermittent fever since two weeks, back pain and walking deficiency started two months before with slow and progressive worsening. Two orthopedic consultations and two back-spine x-rays didn’t report any significant alteration. She was treated with oral ibuprofen for three weeks, with no benefit at all.
In the past medical history she had a Mycoplasma pneumoniae pneumonia when was 16 months-old (diagnosed done through specific antibodies test), treated with oral clarithromycin and clinical healing. No TB cases were reported in the patient’s family.
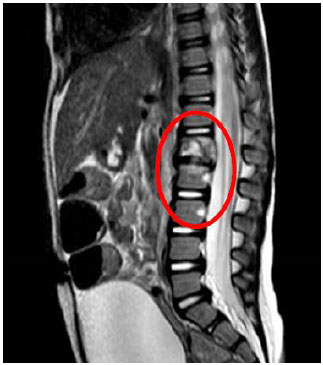
At admission, blood tests showed an increased level of C-Reactive Protein (CRP, 10.8 mg/dL, normal value < 0.5 mg/dL) and leukocytosis (16.800 cells/μL) with neutrophilia (76%). An antibiotic treatment with ceftriaxone was promptly started, with defervescence after two days and mild reduction of CRP and leukocytes, but with persistent back pain and lack of walking. A Mantoux test (positive since 24 hours > 1.5 centimeters) and Quantiferon test (positive) were performed. Chest X-ray, done after these results, showed a small calcific area (probably a lymph node) in the upper part of the right lung. A magnetic resonance of the spine (Fig. 1) showed an extended L1 spondylodiscitis with initial involvement of the upper part of L2. All these data were interpreted as a preview TB infection with a late dissemination and spine involvement.
An anti-tubercular treatment was started with a three-drugs regimen: isoniazid, rifampicin and pyrazinamide. Gastric aspirates, performed before starting anti-tubercular drugs, were negative to Mycobacteria (microscopic examination, PCR and culture). Treatment with pyrazinamide was carried on for two months, whether isoniazid and rifampicin were continued for other 7 months (9 months total).
The patient was also referred to a specialist orthopedic consultation and follow-up, with prescription of a corsept to stabilize the lumbar column.
A magnetic resonance repeated during the follow-up after two months of treatment and at the end did not show any acute sign of spondylodiscitis, with a reduction of both L1 dimensions (body vertebra) and of the inter-somatic space between L1 and L2 (Fig. 2).

We observed a progressive improvement during the follow-up, with a complete remission of the back pain and a progressive improvement in walking. At the last visit (9 months of treatment) the patient was able to walk independently, with a specific orthopedic corsept, and without any neurologic sign.
3. DISCUSSION
In a PubMed review, we looked for all case reports in children in the last 15 years matching the words Pott or Tubercular Spondylodiscitis or Spine Tuberculosis and Children or Pediatric or Infant. In Table 1 are summarized all the single case reports found with this review.
| AUTHOR | CASE REPORT(s) |
|---|---|
| Ng A.W. et al. 2005 [19] (Hong Kong) | Pott’s disease in a 16 years-old-girl complicated with extensive paraspinal abscess. |
| Afzal A. et al. 2006 [20] (Iran) | Pott’s disease and psoas abscess in a 18 years-old-boy. |
| Kiymaz N. et al 2006 [21] (Turkey) | Spinal tuberculosis in a 1 year-old-girl with spinal compression. |
| Du Plessis J. et al. 2008 [22] (South Africa) | Description of 4 pediatric cases of spinal TB. |
| Cassimos D. et al. 2009 [23] (Greece) | Pott’s disease in a two-years old girl. |
| Posner K.R. et al. 2010 [24] (USA) | Pott’s disease unusually presented with sternal mass in a teenage girl. |
| Lee I.C. et al. 2010 [25] (Taiwan) | Cervical spine tuberculosis with abscess in a 13 months-old-child. |
| Consiglieri G. et al. 2011 [26] (USA) | Pott’s disease in a 13-month-old boy. |
| Song D. et al. 2011 [27] (South Korea) | Spinal tuberculosis in a 3 years-old-girl. |
| Kirkman M.A. et al. 2011 [28] (India) | Posterior listhesis of a lumbar vertebra in a 12 years-old-girl with spinal TB. |
| Rangel-Castilla L. et al. 2012 [29] (USA) | Pott’s disease in a 3 years-old-girl with thoracic involvement and surgical treatment. |
| Emir S. et al. 2012 [30] (Turkey) | 3-years old boy with Pott’s disease presenting with Spinal Cord Compression |
| Tian Y. et al. 2013 [31] (China) | Tuberculosis of lower cervical spine in a 24 month-old-boy. |
| Hugar B.S. et al. 2013 [32] (India) | Fatal association between Pott’s disease and retropharyngeal abscess in 13 year-old-female. |
| Katamea T. et al. 2014 [33] (DR Congo) | Congenital spinal gibbosity evoking Pott’s disease in a newborn born to a tubercular mother. |
| Ayuthaya S.I. et al. 2015 [34] (Thailand) | 3 years-old-boy with pulmonary and spinal tuberculosis and Pseudoclavibacter otitis media. |
| Contardo V. et al. 2015 [35] (Chile) | Lumbar Pott’s disease in a 7 years-old-boy. |
| Avcu G. et al. 2015 [36] (Turkey) | Pott’s disease in a 4 years-old-male accidentally discovered after a trauma. |
| Hsin C. et al. 2015 [37] (Taiwan) | Pott’s disease in 13 years-old-boy presented with cold abscess. |
| Papan C. et al. 2017 [38] (Germany) | Pott’s disease and paravertebral abscess in a 16 years-old minor refugee from Somalia. |
| Desnos L. et al. 2017 [39] (French Guyane) | Multifocal tuberculosis in an 11 years-old-girl revealed by spinal tuberculosis. |
Most of the studies that include more patients with Pott’s disease are from developing countries. To the best of our knowledge, the only European case report review comes from the United Kingdom (Eisen S. et al) [7]. They described characteristics of 21 children with Pott’s disease admitted to Great Ormond Street Hospital in a 15 years period (1995 -2010).
In a 6 years study (between 2001 to 2006) Benzagmout M. et al [4] described characteristics and management of 37 Moroccan children (below 15 years of age), in which all of them had a favorable evolution, including patients with initial neurological symptoms and all who necessitated surgical treatment. In another Moroccan study, El Azbaoui S. et al [3], in a prospective observation between 2012 and 2014, described 9 patients with Pott’s disease with a particular attention on relation between IL-12/IFN gamma circuit and radiologic/microbiological data; they did not find any evidence of functional impairment of IL-12/IFN gamma axis in their patients.
In 2001, Ikem I.C. et al [8], in a retrospective 15 years Nigerian study, described characteristics of 34 patients (children and adults) with Pott’s disease: 94.1% of them survived, with a rate of persistent of neurological deficits of 14.7%. In 1995, Beekarun D.D. et al [9], from South Africa, reported 11 children with atypical spinal tuberculosis.
In an African two years multicenter retrospective study, between 1997 to 1998, Rasamoelisoa J.M. et al [10] collected all data on all patients admitted to Tuberculosis in four hospitals in Madagascar: Pott’s diseases was reported in 5% of all patients with Tuberculosis.
In a retrospective 5 years study, from 1999 to 2004, Djientcheu et al [11] described all the characteristics of 43 patients, aged 10 to 69 years old, with Pott’s diseases diagnosed in their center (Cameroon); they highlighted the role of surgery on treatment, in particular in patients with a late diagnosis.
Considering Asian studies, in a retrospective wide and long-term review (between 1971 to 2004), Myung-Sang M. et al [12] described characteristics and management of 124 children with spinal tuberculosis aged 2 to 15 years old in an orthopedic surgery department of a South Korean isle (Jeju).
Al Ayed M. et al [13] reviewed all patients less than 14 years old with central nervous system or spinal tuberculosis diagnosed in a tertiary care center in Saudi Arabia over a 20 years-period. They concluded about safety and utility of brain or spinal biopsy.
Rajasekaran S [14, 15]. in a retrospective Indian study described characteristics of 61 patients with Pott’s disease under 15 years, identifying risk factors to deformity progression: age less than 7 years at the time of disease, thoracolumbar involvement, loss of more than two vertebral bodies and presence of spine-at-risk signs. For these patients, spine stabilization and an accurate follow-up were very important. In another Indian review, Kumar R. et al [16] described characteristics of 19 children with Pott’s disease, with particular attention on the importance of surgical approach for a positive follow-up.
In a 17-years prospective follow-up from Hong Kong, Upadhyay S. et al [17] compared two different surgical approaches on spinal tuberculosis: radical excision or debridement, with better results in the first group.
In a recent report coming from Changsha, China, including 27 children with Pott’s disease, Yin X.H. et al [18] demonstrated a benefit with treatment using percutaneous catheters and low-dose drainage local chemotherapy.
We consider our case report interesting and rare in the same time, due to the origin of the patient (Italy, with no history of contact with TB cases or international travels) and the characteristics of the onset. In a retrospective evaluation, the pneumonia reported when she was 16 months old is now considered tubercular, even if difficult to diagnose considering the epidemiology of the disease and the good outcome she had with oral antibiotic. The positivity of Mycoplasma pneumoniae antibodies leaded also to the misdiagnosis.
Before coming to our attention, the patient suffered from back pain and progressive walking deficiency from two months: this symptom was in our opinion underestimated for a long time, in particular in the orthopedic consultations done, and spine x-ray is not always the gold standard for a right diagnosis, in particular in Pott’s disease. Persistent back pain, especially if associated with a difficulty of walking, has always to be considered a serious red flag in children non-responsive to common treatments.
CONCLUSIONS
Pott’s disease is the most common type of skeletal manifestation of TB. Very rare in non-endemic countries, this manifestation is more probable in children than in adults. To the best of our knowledge, the case report we reported is the youngest Italian patient with Pott’s disease described in the literature.
Diagnosis of tubercular spondylodiscitis in children coming from developed countries, with no history of TB and travel or living in poor condition, is rare and very difficult, but an early recognition could lead to a positive outcome. The incidence of TB is increasing in developing countries, mostly due to immigration.
Back pain, in particular when associated with walking deficiency, has to be considered a serious problem in children with no benefits from common treatments.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
A written informed consent was obtained from all patients when they were enrolled.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none

