All published articles of this journal are available on ScienceDirect.

Very Long Persistence of Botulinum Toxin B in a Patient’s Serum
Authors Info & Affiliations
Abstract
Background:
Botulinum toxins (BoNT) type A, B, E, F may induce a serious neuroparalytic illness in humans. Botulism can be transmitted via three routes: foodborne, wound and intestinal (in situ toxemia generally observed in infants and/or in immunocompromised adults) botulism.
Case Report:
A case of human botulism type B due to the consumption of an imported dried ham is reported. Laboratory results confirmed the diagnosis using the mouse bioassay and the qPCR method. Botulinum toxin was still detected in the serum up to 29 days after food consumption while it was not detected anymore in the faeces.
Conclusion:
The described case highlights i) prolonged presence of BoNT B in the serum and ii) the risks related to the preparation of artisanal products as well as the importance of an efficient communication to citizens regarding preservation methods of household products.
1. INTRODUCTION
Human botulism is rare with only 19 cases reported in Belgium from 1988 to 2016 (data from the National Reference Centre, NRC). We describe the investigation of a case that occurred in March 2015 following the consumption of dried ham purchased in Romania. The patient presented typical bilateral cranial nerve impairment. Human samples (stool and serum) and two leftover hams were analysed at the NRC. The presence and identification of neurotoxins was assessed using the mouse bioassay (Ethic agreement n°20140808-01). Food and faeces samples were extracted and cultured in enrichment media, as adapted from [1]. A real-time PCR assay (qPCR) was performed on DNA extracted from the enriched cultures in order to detect the presence of BoNT genes as adapted from [2].
Laboratory tests confirmed clinical diagnosis of botulism. Because the sister of the patient unveiled a previous botulism case eight years before, the patient’s condition was carefully followed. The public health officials of Infectious Diseases Control sent therefore consecutive samples for laboratory analyses. The presence of the toxin in the serum as well as the faecal excretion of the germ and the toxin were carefully monitored.
2. CASE REPORT
2.1. Epidemiological Investigation
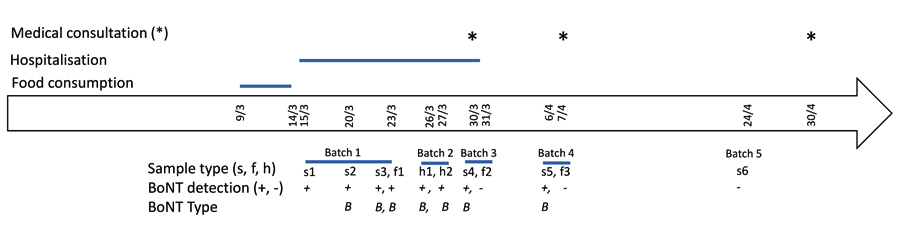
Artisanal ham bought in Romania was brought back by the patients’ sister in December 2014. The food was consumed during January and February 2015 by the sister’s husband and son, without them manifesting any symptom. The patient ate slices of dried ham every day in the second week of March. The onset of symptoms occurred on March 14th and consisted of blurred vision, difficulty in swallowing, dry mouth, oesophagus problems and mydriasis. As summarised in Fig. (1), the patient was hospitalised on March 15th, discharged from hospital on March 31st and was then asked to provide frequent biological samples. On April 30th, the health status of the patient was good, with the only persisting complaint being a low stool frequency. A total weight loss of 7 kg was noted. In January 2016, the patient still complained of a tingling sensation in arms and legs as well as a dry skin.
2.2. Laboratory Investigation
Five batches of samples were sent to the laboratory (Fig. 1) for detection of BoNT and/or BoNT-producing C. botulinum. Positive results were obtained until the last batch received on April 24th which turned out negative (Table 1).
|
Batch n°/ Sample n° |
Sampling Date | Mouse Bioassay (MBA)1 + Seroneutralisation (SN) and Enrichment followed by qPCR | Result without/with Seroneutralisation (SN)2 | Conclusion |
|---|---|---|---|---|
| 1/ Serum 1 | 15-March | BoNT (MBA) + SN ABE-F | † / - | BoNT detected |
| 1/ Serum 2 | 20-March | BoNT (MBA) + SN B | †/ - | BoNT B detected |
| 1/ Serum 3 | 23-March | BoNT (MBA) + SN B | † / - | BoNT B detected |
| 1/ Faeces 1 | 23-March | BoNT (MBA) + SN ABE-F | † / † (non specific) | BoNT Not detected |
| C. botulinum (MBA after enrichment) | negative | BoNT Not detected | ||
| BoNT gene (qPCR) | + | C. botulinum type B | ||
| 2/ Ham (small) | 26-March | BoNT (MBA with trypsin treatment) | † | BoNT detected |
| C. botulinum (MBA after enrichment) + SN B | †/ - | BoNT B producing-C. botulinum | ||
| BoNT gene (qPCR) | + | C. botulinum type B | ||
| 2/ Ham (big) | 27-March | BoNT (MBA with trypsin treatment) | † | BoNT detected |
| C. botulinum (MBA after enrichment) + SN B | †/ - | BoNT B producing-C. botulinum | ||
| BoNT gene (qPCR) | + | C. botulinum type B | ||
| 3/ Serum 4 | 30-March | BoNT (MBA) + SN B | specific mild symptoms 1, 2, 3 | BoNT B detected |
| 3/ Faeces 2 | 31-March | BoNT (MBA) | - | BoNT Not detected |
| C. botulinum (MBA after enrichment) | - | BoNT Not detected | ||
| BoNT gene (qPCR) | - | BoNT Not detected | ||
| 4/ Serum 5 | 6-Apr | BoNT (MBA) + SN B | specific mild symptoms 1, 2, 3 | BoNT B detected |
| 4/ Faeces 3 | 7-Apr | BoNT (MBA) | - | BoNT Not detected |
| C. botulinum (MBA after enrichment) | - | BoNT Not detected | ||
| BoNT gene (qPCR) | - | BoNT Not detected | ||
| 5/ Serum 6 | 21-Apr | BoNT (MBA) | - | BoNT Not detected |
2 -: no symptom, † death or specific signs compatible for botulism 1 for visible abdominal hypotonicity, 2 for touch abdominal hypotonicity, 3 for the characteristic wasp size (retracting the abdomen) .
All serum samples from the first batch induced death in inoculated mice and the toxin type B was identified. The faeces from the same batch induced death in mice but, surprisingly, the seroneutralisation was unsuccessful. This indicated that other potential toxic compounds could not be seroneutralised in the faeces inducing non-specific reactions in mice, as mentioned in [1]. However, the presence of C. botulinum containing a BoNT/B gene was confirmed by the qPCR assay.
BoNT B was detected in the two ham samples after addition of trypsin. Accordingly, the enriched cultures resulted positive for the presence of BoNT B-producing C. botulinum either by the qPCR assay or by the mouse bioassay.
The third and fourth batches of sera showed similar but weaker positive results than the first batch and did not lead to death in mice. The toxin type B was identified in all samples. The two faeces resulted totally negative (Table 1). Sample of the last batch resulted negative.
3. DISCUSSION
A thorough follow-up of the patient has been performed. All the serum samples, except for the last one, were positive for BoNT B, as determined by the bioassay. A decrease in toxicity was observed with time, along with the gradual decrease of clinical symptoms. But the toxin type B was still detectable in the serum 29 days after consumption of the contaminated ham which is the longest persistence in serum ever demonstrated for foodborne botulism. It can be hypothesized that the patient ingested spores of C. botulinum by eating the contaminated ham, then underwent an in situ toxin production. The last sample taken more than one month after the hospitalisation date, turned out negative indicating the end of toxin circulation in the patient’s body.
The uptake of BoNT and C. botulinum by the patient had been stopped during hospitalisation though the toxin was still detected in serum long after his discharge. The persistence of circulating toxin in serum has been scarcely documented whereas excretion of toxin in the faeces is common. Fagan and co-workers [3, 4] described two individual cases for which a toxin-positive serum was obtained 11 days after ingestion of contaminated food in a type B outbreak and 24 days after hospitalisation in a type F botulism rebound case, respectively. The relapse was due to the intestinal colonization of BoNT F-producing Clostridium in the patient’s body. Here, the toxin was still detectable in the serum 22 days after hospitalisation.
Interestingly, the toxin could not be detected in the faeces from the first batch although presence of C. botulinum containing a BoNT/B gene was shown by qPCR assay. This would suggest that the toxin was either not excreted at detectable levels in the faeces, that other toxic compounds may interfere with the MBA or that solely cell-free DNA was detected in qPCR. Moreover, in the cultured faeces, the growth of C. botulinum was likely inhibited by background flora explaining the absence of toxin detection in the culture of faeces. The faeces from next batches resulted negative by all the performed tests. In the rebound case type F [4], stool enrichment cultures tested positive for BoNT F on day 29 after hospitalisation but were found negative after day 30. In our case, such prolonged excretion in faeces was not observed although the toxin was still present in the serum. A recent study suggests that the persistence of BoNT intoxication can be influenced both by the ability of the toxin protease or its cleaved SNARE protein substrate to resist turnover [5].
The two dried ham samples resulted positive for BoNT B after trypsin treatment. A BoNT B-producing C. botulinum was detected in cultured ham by the qPCR assay and by the bioassay. This means that the patient ingested both BoNT and spores/cells of C. botulinum, the latter being a group II strain (non-proteolytic) which requires full activation of its toxin by trypsination as it occurs naturally in the human digestive tract.
The presence of group II C. botulinum in protein rich foods poses some concerns due to its optimal growth temperature ranging between 18-25°C and the minimal temperature required for toxin production (only 3°C), conditions which are easily met in a household environment. Furthermore, there is no particular smell when foodstuff is contaminated with non-proteolytic C. botulinum, as in this case.
Adult intestinal toxaemia is caused by rarely occurring intestinal colonization of BoNT-producing Clostridia [3], with prolonged in situ production of BoNT. Adult intestinal toxaemia generally occurs in immunocompromised people or in people who present a weakened intestinal flora, e.g. after recent antimicrobial treatments or gastrointestinal abnormalities. To our knowledge, this was not the case for the patient. The persistence of BoNT B in the patient's serum for at least a month after onset of illness supports similar diagnosis although the absence of toxin detection in faeces as well as the decreased concentration of toxin in the serum impairs that hypothesis.
However, it cannot be excluded that, besides the lack of competing flora, other factors can influence the susceptibility of the patient as, for instance, a genetic predisposition to botulism in the family. Indeed, eight years ago, the patient’s sister experienced a botulism episode. Among all the exposed people, she was the only one who turned ill. Unfortunately, the serotype was not determined. She still experiences today dry skin and mouth, and a burning sensation in arms and legs. Although her husband and son also consumed the contaminated ham frequently, only her brother (the patient) suffered from the herein described botulism. The onset of botulism symptoms is certainly related to the amount of toxin that has been ingested by the patient. Unfortunately, the exact amount ingested by the three individuals is not known.
The mild clinical symptoms as well as the possible adverse drug reactions made general practitioners decide not to administer antitoxin neither antibiotics. At our last follow up, 1.5 month after diagnosis, the patient still had some minor complaints (i.e. a tingling sensation in arms and legs and dry skin). However, the demonstrated long persistence of the toxin in the serum indicates that antitoxin treatment may be administered longer after exposure than previously thought (treatment as soon as possible being currently advised).
CONCLUSION
In conclusion this report illustrates a confirmed case of botulism type B with prolonged presence of BoNT B in the patient’s serum. The risks related to the preparation of artisanal products, especially in case of presence of non-proteolytic C. botulinum and the necessity of defining the window for giving antitoxin treatment are highlighted.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The procedure of botulinum toxin analysis using the mouse bioassay has been submitted to the ethics committee (Ethical Committee of the CODA-CERVA/WIV-ISP) and has been approved under the n° 20140808-01.
Authorization has been accorded on November, 17th, 2014 for use of mouse testing for toxin detection.
HUMAN AND ANIMAL RIGHTS
No humans were used in the study. Sciensano follows the recommendations of the Belgian Royal Decree of May 29th 2013 linked to the European 2010/63/UE Directive of 22 September 2010 on guidelines for accommodation and care of animals used for experimental and other scientific purposes. All care and use of laboratory animals were followed.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICTS OF INTEREST
The authors declare that there is no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We acknowledge the technical staff members, Francis Tweepenninckx and Laurie Flament, who performed the laboratory investigations. Inspectors of the Federal Agency for Safety of the Food Chain and Inspectors of the Health Inspection are gratefully acknowledged for the collection of samples and excellent collaboration.

